


Paradigms, processes, and payment
An assessment of leverage points, 2 years in

This organisation has a goal–to transform the psychiatric crisis system so it works for people. Last year, after a year of investigation, I concluded that the next step in the process was establishing a crisis service this organisation controlled, so we could experiment with different structures, cultural norms, and ways of relating to people, in order to find something that worked for anyone at all.
We’re currently in the final stages of a bidding process to run a mobile crisis service for a twin-county region in California. I partnered with two experienced crisis response leaders who used to work at CAHOOTS, a non-police mobile crisis response service that has been active in Oregon for many decades longer than almost all other crisis teams. We will know shortly if we were chosen, and if so, the work can begin.
I also got appointed to serve on the California Behavioral Health Planning Council, which advises the state health department on how the system is working and how to improve it. I’ll say more about that in a related post, but one result of this appointment is I’ve gotten a much closer look at the workings of government and its paradigm and culture with respect to mental health than I’d previously had. This has given me a better sense of what the government-led system can and cannot do, and where its blindspots might be.
All of this (as well as now having a -way- better picture of the regulatory limitations surrounding any attempts to build parallel systems as a result of bidding on contracts to build crisis programs for counties) has crystallised in my mind the shape of the landscape with respect to the socio-structural change that is likely required and might be possible, in order to unfuck crisis care.
One way to think about this is–what are the dependencies in this enormous system? And, given those dependencies, where does change need to start in order to flow to all the necessary parts of the system?
In particular, power flows hierarchically in most of the relevant institutions, and in some specific lateral ways, where one institution holds a particular kind of authority over another. This ties the system together in a way that makes most participants in it feel relatively powerless except in a few specific cases.
Despite the scandals of the replication crisis and the lack of on-the-ground research modalities in psychological, neuroscience and psychiatric research, it’s still the case that most practitioners inherit the paradigm they operate within from the scientific research industry, which itself is most influenced by the work of the most prestigious research institutions. Trying to change the mindset of practitioners who work for the government directly looks like a futile endeavour because ‘changing paradigms’ is not part of their job description–in fact it may conflict with the requirements of their job description.
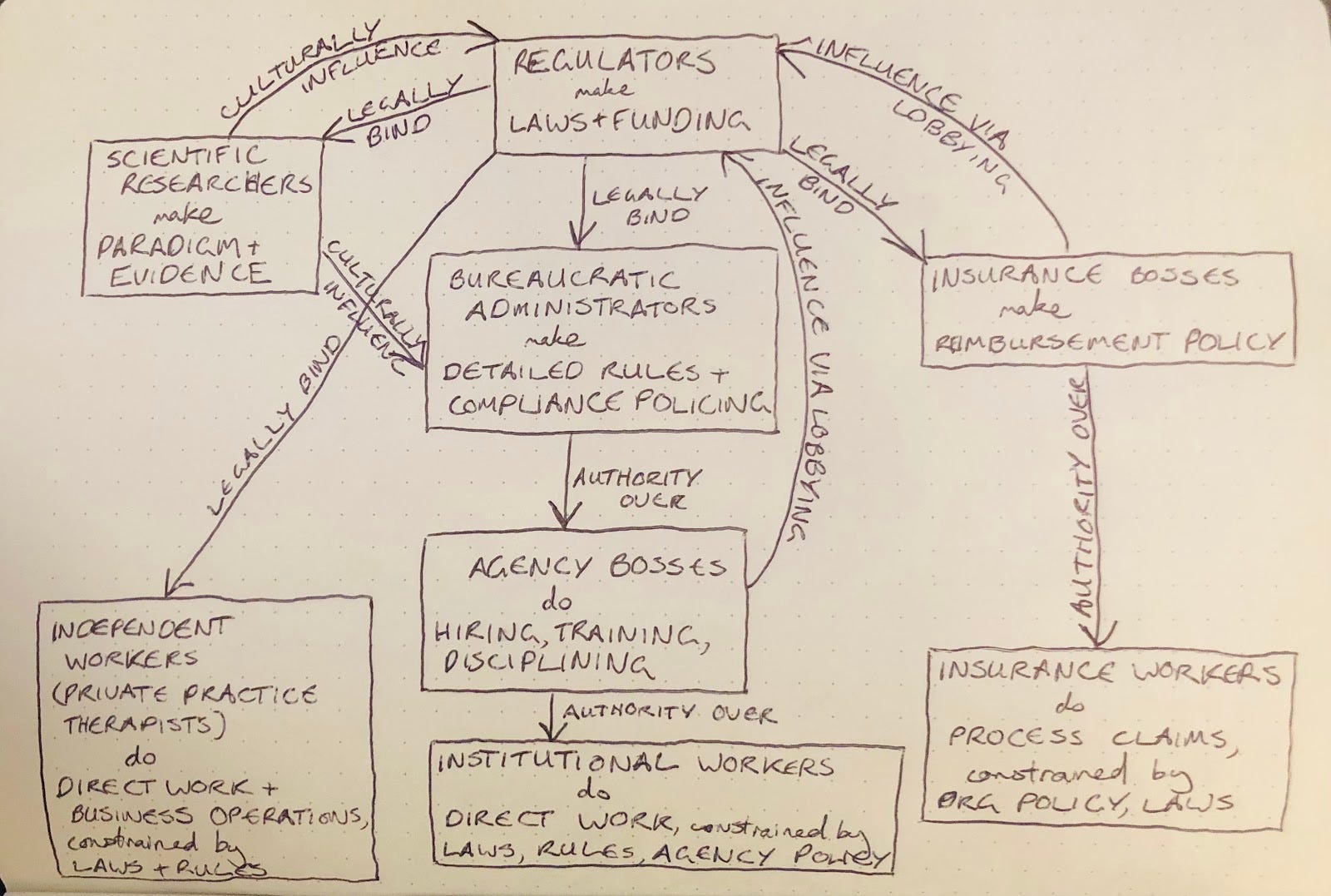
(A hastily-made diagram of how I see the power flows amongst the various institutions and groups responsible for maintaining the mental health system. Describes the state system in California more than anywhere else, but I think it somewhat generalises to other places. Definitely wrong, maybe useful.)
As a result of this investigation I think these are the three leverage points which are necessary (but perhaps not sufficient) for shifting the mental health system in western countries into a new, better, stable system state. They’re sort of coupled, hierarchically–the first leverage point influencing the second and third, and the second influencing the third.
Behold:
(1) Expand the shared neuro/psych research paradigm beyond purely-empirical scientific materialism to something better suited to the personal, subjective nature of psyches, minds, souls, people
Modern psychology and psychiatry relies on scientific research in psychology, medicine, psychiatry and neuroscience to create and refine knowledge about how minds work and how best to treat their problems. Almost all of this research (and all of the most prestigious or highly-regarded research) relies on an a paradigm about ontology and epistemology (what is real and how we can know anything) that assumes that everything is made up of a bunch of physical stuff, and that any non-material phenomena is irrelevant. It’s closely connected to an epistemological philosophy that regards experimental research to be the only major, if not the only legitimate source of knowledge about minds, people, emotions, and mental phenomena, and considers only knowledge that is universally generalisable to be valid and worth pursuing.
This paradigm excludes all that is idiosyncratic, illegible, physiological but systemic or subtle or idiopathic, not measurable in physical or literal terms, personally experienced (unless transformed into generalisable knowledge), hidden or taboo, or subjectively or inter-subjectively meaningful. The paradigm also does not attempt to make sense of vast swathes of what is and has historically been important to those who practise religions–ideas of divinity, deities, souls, ethics, eschatology (amongst others)--ideas which have historically been very important to mental and emotional wellbeing. Because of this, this paradigm is ill-suited to supporting the care of people’s minds, emotional lives, spirits, souls, and sense of self and personhood.
Because of the replication crisis, a small but influential chunk of people who work in research psychology, psychiatry and other fields now recognise the large gap between the reliable knowledge the scientific research community promises and the practices of psychology, psychiatry and other fields of mental health care.
A new paradigm would better reconcile all the subjective and intersubjective dimensions currently excluded from the dominant scientific materialist psychology, psychiatry, neuroscience research paradigm with the practical needs of those who do caring work for people with mental and emotional problems, as well as those who administer and fund the work. It would be more useful for implementing large-scale strategies that help lots of people recover from crises and chronic problems.
(ChatGPT informs me that some other major paradigm shifts in scientific disciplines took about a century; perhaps with faster information flows in our time a paradigm shift might be quicker? But it’s impossible to say.)
(2) Reform bureaucracies to be better suited to the task of administering mental and emotional (and spiritual) care
Bureaucracies administer the vast majority of professionalised mental and emotional care today, and almost all of the care for people whose problems are considered especially dire. These bureaucracies are mostly county and state government departments, insurance companies, including managed care organisations, hospitals, and large social services agencies and other nonprofits who receive government funding.
They operate on a basic process of:
High-up leaders identifying the problem to be solved
High-up leaders formulating an imagined solution to the problem, perhaps after listening to those more ‘on-the-ground’ (lower in the hierarchy, or those actually experiencing the problem directly)
Higher-up leaders breaking tasks into parts and assigning those parts to lower-down people or departments
Higher-up leaders evaluating the lower-down groups by how faithfully they adhere to the plan that they were assigned
The higher-ups being punished or rewarded by -their- higher-ups according to how faithfully the plan was adhered to
(This is still the case if the higher-ups are in a separate organisation and the lower-downs are receiving a grant, for example–the structure is about who is allowed to punish or reward whom, not who is in the same organisation.)
This model of work assumes that the problems in question are a certain shape–that they are well-defined, that they can be understood using reasoning/rationality at scale, that they can be solved by programmatically-implemented solutions, and that progress on the problem as a whole can be measured by aggregating measurements of progress in the parts. Sadly, none of this is true about ‘the mental health crisis’. Modern bureaucratic administrative techniques are a terrible fit for this problem.
These techniques are not an amazing fit for several kinds of problems (particularly social ones), but are especially problematic when it comes to personal mental and emotional care–which tends to be relational, private, and idiosyncratic, involving multiple spheres for a given individual that cannot be decoupled. As a result, administrative leaders are forced to formulate weak concepts, to command the completion of ineffective tasks, and to evaluate the completion of tasks independent of their input towards the stated goal.
This is bad for everyone–the leaders are charged with authority but aren’t practically connected enough to the various situations where the problem is found to create plans that will address the varied demands of each situation, the employees are limited in their agency, and are often forced to keep carrying out plans even when they don’t seem to be helping. Employees, in order to have successful careers, tend to try to climb the ladder of hierarchy, thereby draining the ‘ground-level’ of people who might be really good at solving the problem.
The field of software development mostly moved on from a paradigm like this (called ‘Waterfall Development’) years ago in favour of something called Agile, which emphasises flexibility and adapting the plan to incorporate knowledge gained through the creation process. I think a similar sort of paradigm shift is required in the administration of mental health care–although the paradigm will not be identical to Agile, as Agile is adapted to the needs and constraints of the software industry.
(ChatGPT gives examples of shifts like this in bureaucratic administration styles that took a few decades; in some cases, only 20-30 years. In many cases they were led by the head of state.)
(3) Using (1) and (2), reform the way caring work is priced, categorised and contracted so it is better suited to the idiosyncratic/idiopathic nature of peoples’ personal crises
What work can happen, who does it, how reliable it is to the patient, and how well-suited it is to the patient’s situation is strongly affected by how the work is defined and agreed upon so it can be paid for. The constraints of funding are affected by the motivations and capabilities of private insurance companies, public insurance companies, and billing departments, and affected by things like how billing codes work and which occupational licences are associated with which payouts.
Current payment agreements and processes often work against the needs of the patient and the situation and make it harder than it needs to be. This is partially because of the influence of the scientific paradigm and administrative paradigms above.
The work of transforming the scientific and administrative paradigms from (1) and (2) must be translated into different, sustainable agreements and processes around approving and funding care work to help someone experiencing mental and emotional problems.
Other problems that also pose a risk, but don’t seem to be more important leverage points than the first three approaches:
All the major public mental health administrations are experiencing a large shortage of workers, particularly for jobs involving a lot of face-to-face, physically risky contact. So, even if all these problems were satisfyingly addressed, there may be no one willing to do the work based on them.
There’s a general breakdown in how well public bureaucracies (in America) can implement policies, even once they are agreed upon. So, if policy changes are required in order to change the payment process or research funding processes, these policy changes might not be successful.
The ability of government bureaucracies to continue administering and for private healthcare and insurance companies to continue operating relies on civil stability and the peace afforded by uncompromised national sovereignty. In the event of war or serious civil unrest (or, in areas where that is already present or likely), it might become difficult to impossible to keep operating a mental health system.
There are some class and implicit-social-contract-related factors that seem to strongly influence things about people’s minds and what good and bad mental health looks like, and these seem pretty taboo in the scientific, bureaucratic and therapeutic communities. So, this could get in the way of good theory development, and good administrative reformulation.
A bunch of laws are currently in place that have at best ineffective and at worse counterproductive effects on the sanity and mental wellbeing of the people they statedly serve. If they stay in place long term, they might counteract any benefits from improved paradigms or processes.
These three leverage points currently guide my thinking about what opportunities to look for for Psych Crisis (aside from the potential in-person crisis program.)
Very few people, if any, are operating directly on the three leverage points above. For most people in the business of attempting to ‘fix the mental health system’ these leverage points are not even on their radar. I think they’re tractable, given a long enough time-scale, and the effort of enough skilled, devoted people (not that I know what that number is).
What do you think? For those who work in the system, how does this reflect your experience?
(P.S. I got married! My name is now Jessica Ocean.)